Digital transformation and social networking sites have opened more ways than ever for the MSM community to meet sexual partners1. It has also been found that MSMs active on virtual platforms are associated with higher risk of HIV compared to those using only physical sites2. Thus, HIV programs need to integrate novel methods to respond to the dynamic needs and networks among MSMs.
HIV prevalence among MSM in the National Capital Territory of Delhi (Delhi NCT) has declined from 5.3% in 2010-11 to 1.8% in 2017; however, it is much higher than the national adult general population prevalence of 0.3%. National AIDS Control Organization (NACO) has been consistently working towards prevention of new infections in the Key Populations and is designing and implementing various strategies to control the spread of HIV in India through the Targeted Intervention (TI) program. NACO has been implementing exclusive Targeted Interventions for MSMs with 11 TIs in Delhi reaching out to 16052 MSMs in Delhi3.
Discussions and interactions with the MSM community by the MSM TIs in Delhi highlighted the growing usage of virtual platforms like social networking sites, messenger groups, dating applications, among others, by the MSM community for solicitation. As per site validation 2014 done by NACO, there are 18145 MSMs in the state; however as indicated by the virtual mapping exercise, the actual number of MSM is much higher. According to the virtual mapping exercise conducted by Delhi State AIDS Control Society (DSACS) in collaboration with Delhi Technical Support Unit (DL TSU), an estimated number of 28058 MSMs use various virtual sites to meet other MSMs. The mapping exercise highlighted the active presence of MSMs on virtual platforms and signalled the need for a strategy to encompass the population active on virtual platforms under the TI program. This led to the development of virtual interventions with the MSMs in Delhi NCT that would reach out to those who operate on the virtual platforms, provide TI services to them and motivate them to access the facilities of HIV/ AIDS, STI screening on regular basis and to initiate and adhere to treatment, when HIV infected.
This virtual intervention aimed to identify and link the MSMs using virtual platforms with the HIV services. The objectives of virtual intervention were:
In India, to date, limited evidence exists on virtual interventions. The Virtual Intervention for MSM in Delhi is one such endeavor that can be considered as the first government-led and cost-effective intervention incorporated in the existing TI program, that provides HIV prevention, care and treatment services to MSMs active on virtual platforms.
This intervention has been rolled out with 11 TIs dealing with the MSM community in Delhi NCT. All the eleven districts of Delhi NCT, namely, North Delhi, North East Delhi, North West Delhi, South Delhi, South East Delhi, West Delhi, Central Delhi, New Delhi, South West Delhi, Shahadra and East have been covered under this intervention.
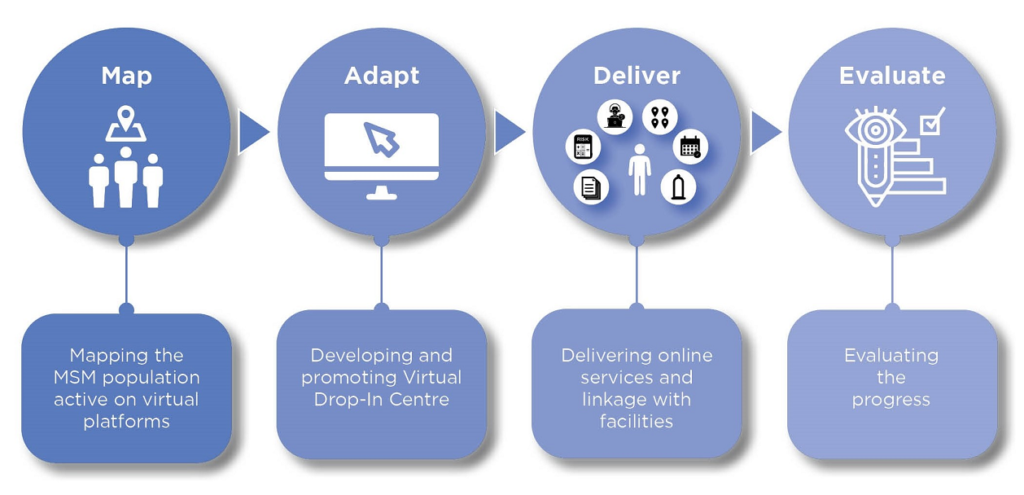
The intervention was implemented through the MADE Model – Map, Adapt, Deliver and Evaluate (Figure 1). This innovative model is an evidence based practice used to Map the MSM population active on virtual platforms, Adapt the services to a digital mode for increasing the reach, Deliver the services to the community and Evaluate the progress and also provide handhold support to the TIs in implementing the Virtual Intervention to encourage more and more community members to access the services (Figure 1). This model is an excellent example of co-development through community involvement and participation. It substantiates the approach ‘of the community, for the community and by the community’.
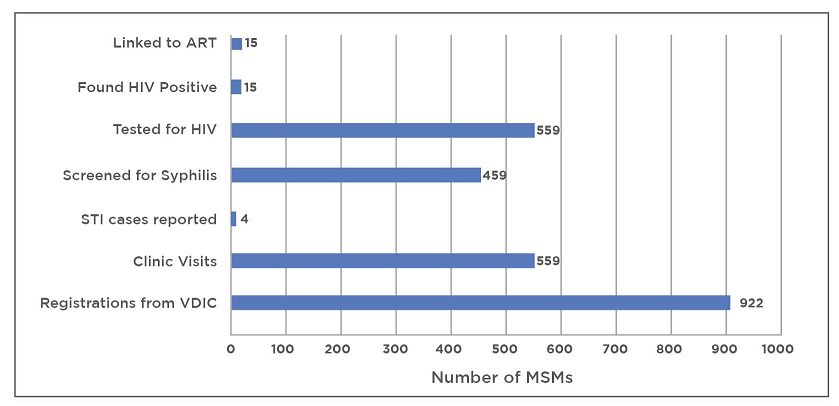
The progress of the intervention has been captured through data pertaining to access of VDIC services by the MSM community and consequent linkage with TI and Health Facilities. From November 2018 till March 2020, 922 MSMs active on virtual platforms were reached through Virtual Interventions, which includes VDIC as well as online outreach activities. They have registered in TI. Out of these, 559 MSMs have visited TI static clinic for STI check-up and counseling; same number of MSMs underwent HIV testing and 459 MSMs were screened for Syphilis. HIV and Syphilis testing services were provided to them at the doorstep or at TI or at a location convenient to them. While 4 MSMs were reported to have STI; 15 MSMs tested HIV positive and have been linked to ART centre and are currently undergoing treatment (Figure 3).
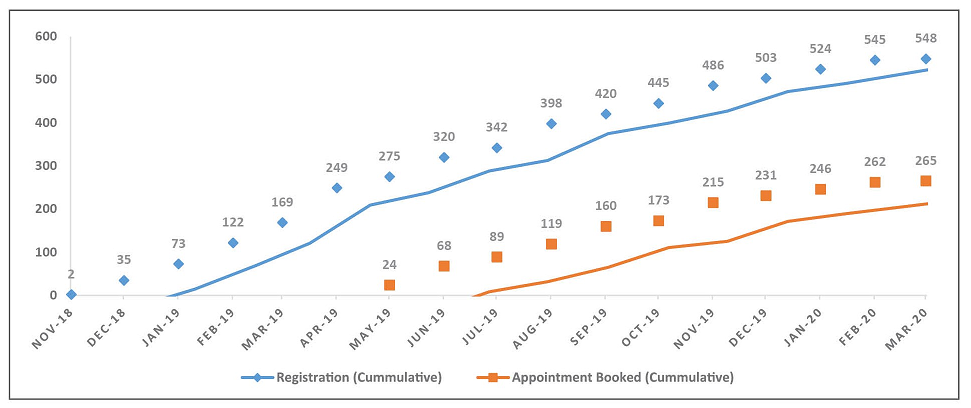
Out of 922 MSMs, 548 MSMs have registered in the TI through VDIC. Out of them, 265 had availed services from STI clinic, TI program, ICTC and ART centre, as per their need. Out of the 26 MSMs, 104 MSMs took appointment for HIV testing. While not all who have registered through VDIC have taken appointments, we can observe a gradual increase in registrations as well as appointments (Figure 4).
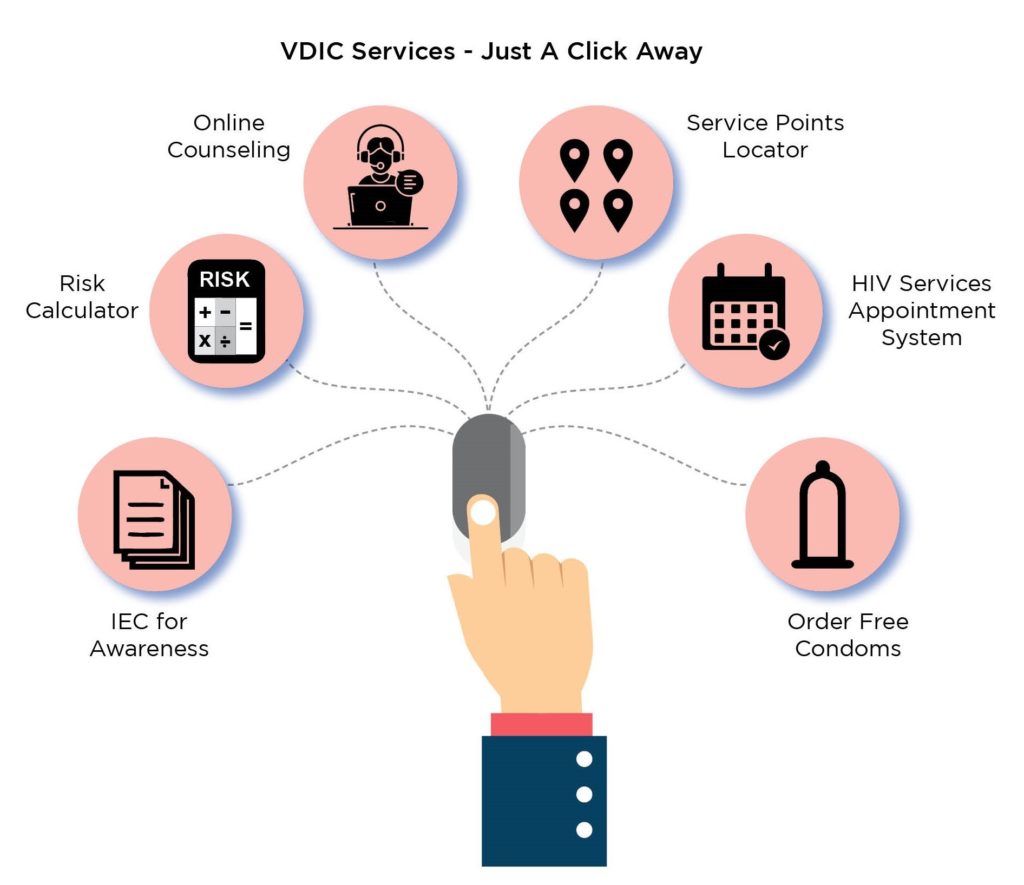
Virtual Interventions are a promising innovation that use virtual tools to reach out to MSMs and link them to HIV services. The community has provided an affirming feedback for the VDIC as some of the services are just at the click of a button and confidentiality of the user is maintained. As the TI program comprehends the VDIC benefits, applicability and impact that it is creating, the intervention can be strengthened and taken to the next level.
In order to reach out to the community and make the platform user-friendly, the VDIC will be accessible and compatible on mobile devices in the form of application. The intervention will also focus on promotion of the VDIC platform to bring visibility to the services offered. Further, it also seeks to take up some innovative initiatives to strengthen its service delivery and at the same time saturate the population in order to bring every individual community member under its purview.
1 Mapping and Size Estimation of MSMs active on Virtual Platforms in Delhi, IHAT, DSACS, 2020
3 Targeted Intervention Program Data (Year 2019-2020)